ARTHROSCOPIC MENISCAL SURGERY
MENISCECTOMY - MENISCAL REPAIR
ROLE OF THE MENISCI
The menisci are crucial structures in the knee, made of strong cartilage and located between the femur (thigh bone) and the tibia (shin bone). They have several important functions in the knee:
- Cushioning : The menisci act as natural shock absorbers, distributing the pressure placed on the knee during walking, running and other physical activities. They help absorb shock and prevent premature wear of joint cartilage.
- Stability : The menisci help stabilize the knee by evenly distributing the load across the joint surface. This helps prevent excessive sliding or displacement of the joint surfaces, which is essential for proper knee function.
- Load distribution : By distributing the load over the entire surface of the articular cartilage, the menisci help to avoid excessive concentration of pressure on certain areas of the knee. This helps prevent uneven wear of the cartilage and reduces the risk of developing osteoarthritis.
- Improved joint congruence : The menisci contribute to better joint congruence, that is, the precise fit and coordination of the joint surfaces of the femur and tibia. This promotes smooth movement and reduces friction between bones.
- Lubrication : The menisci help lubricate the knee by producing synovial fluid which reduces friction between the joint surfaces. This facilitates movement and preserves cartilage health.
The menisci play a vital role in maintaining the function, stability and overall health of the knee. In cases of meniscal damage, surgical procedures such as meniscectomy or meniscal suture may be necessary to restore normal knee function.
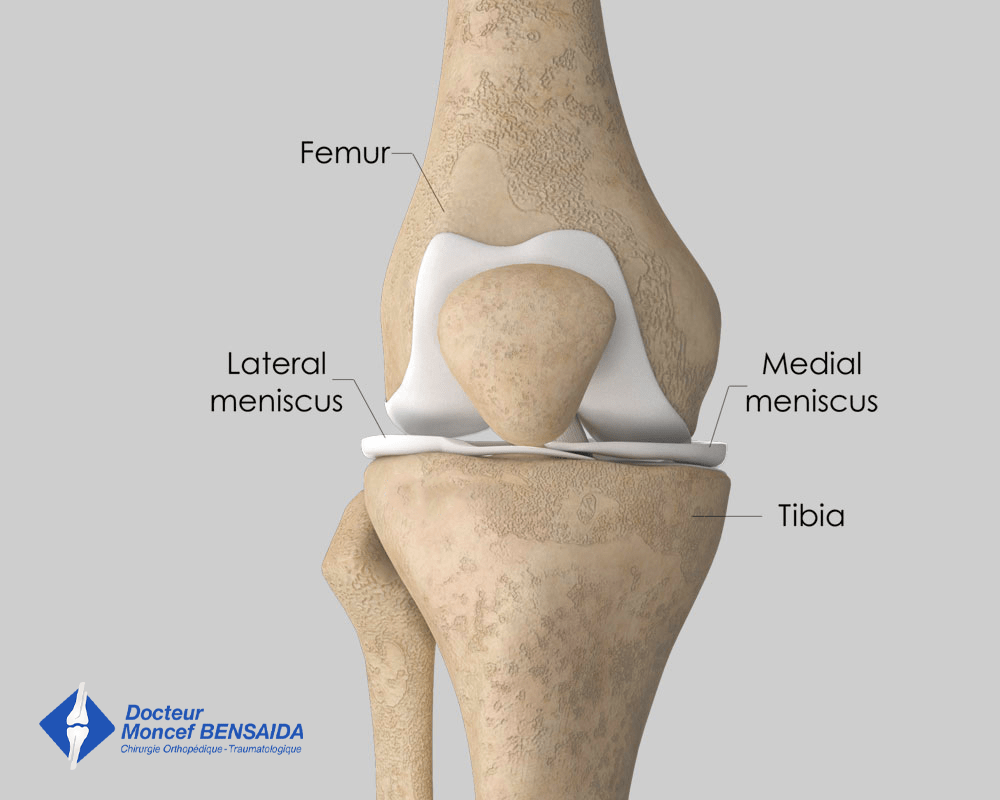
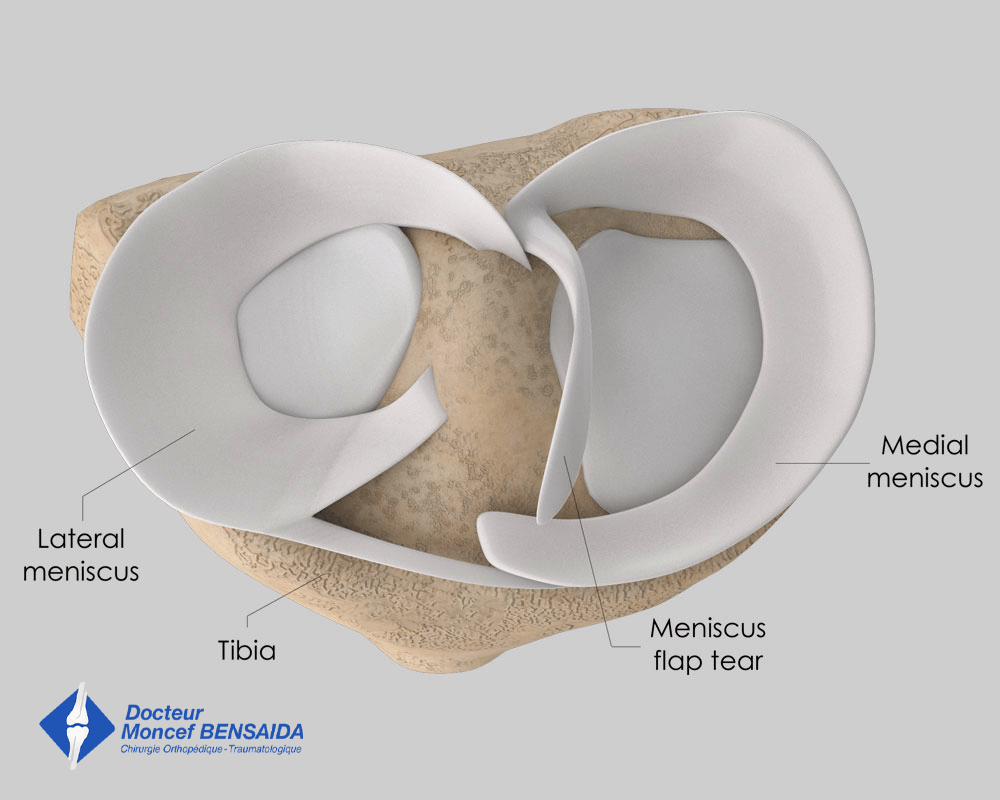
Meniscus anatomy
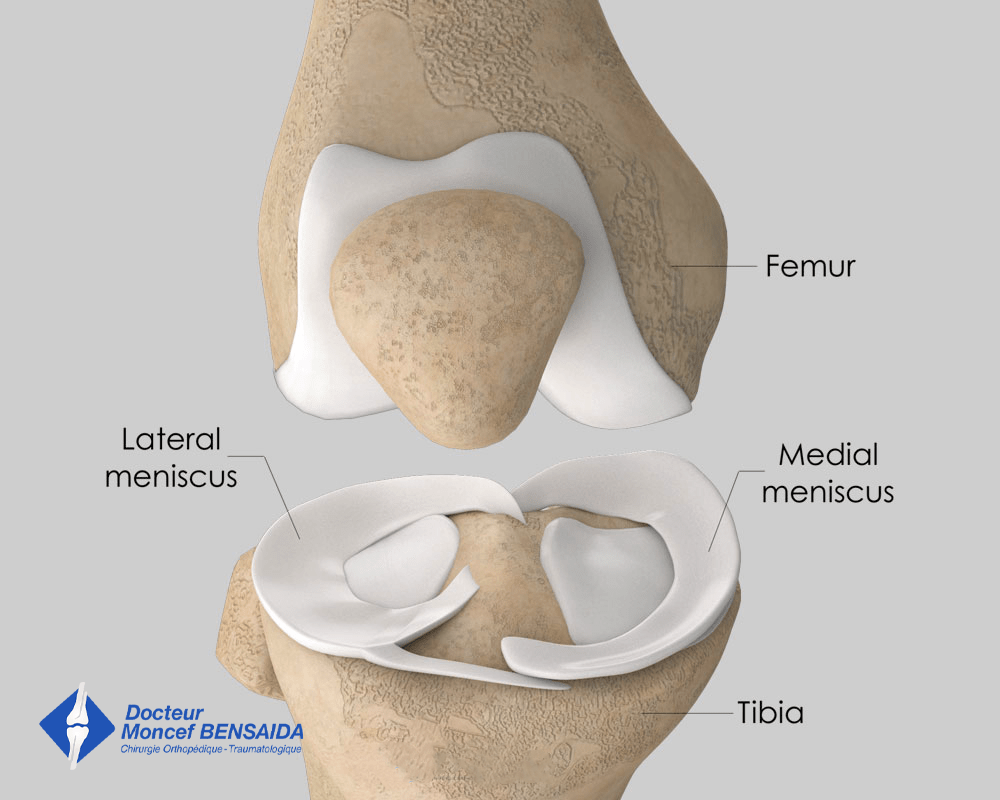
Meniscus anatomy
DIFFERENT TYPES OF MENISCAL TEAR
In some circumstances the meniscus can tear. This damage can be distinguished according to 2 criteria: the cause (trauma or degenerative) and the stability (with or without a mobile meniscal fragment).
Meniscal damage can occur at any age but its nature differs according to the age of the subject.
In patients under 40, meniscal damage is often caused by trauma resulting from a one-off excess load on the meniscus occurring during a sports activity or when crouching. When these traumas occur, the meniscal damage may be associated with knee ligament damage such as an anterior cruciate ligament tear.
In older patients, meniscal damage is more often degenerative. As the meniscus gets older it weakens and can tear during quite insignificant movements, not at all during sports activities. This aging of the menisci is an integral part of knee ageing and begins in your forties. It is not uncommon that degenerative meniscal damage is associated with knee osteoarthritis.
Furthermore, some meniscal lesions can result in abnormal movement of the torn part of the meniscus. These unstable lesions can result in the knee giving way and even locking, as well as not being able to completely straighten the knee.
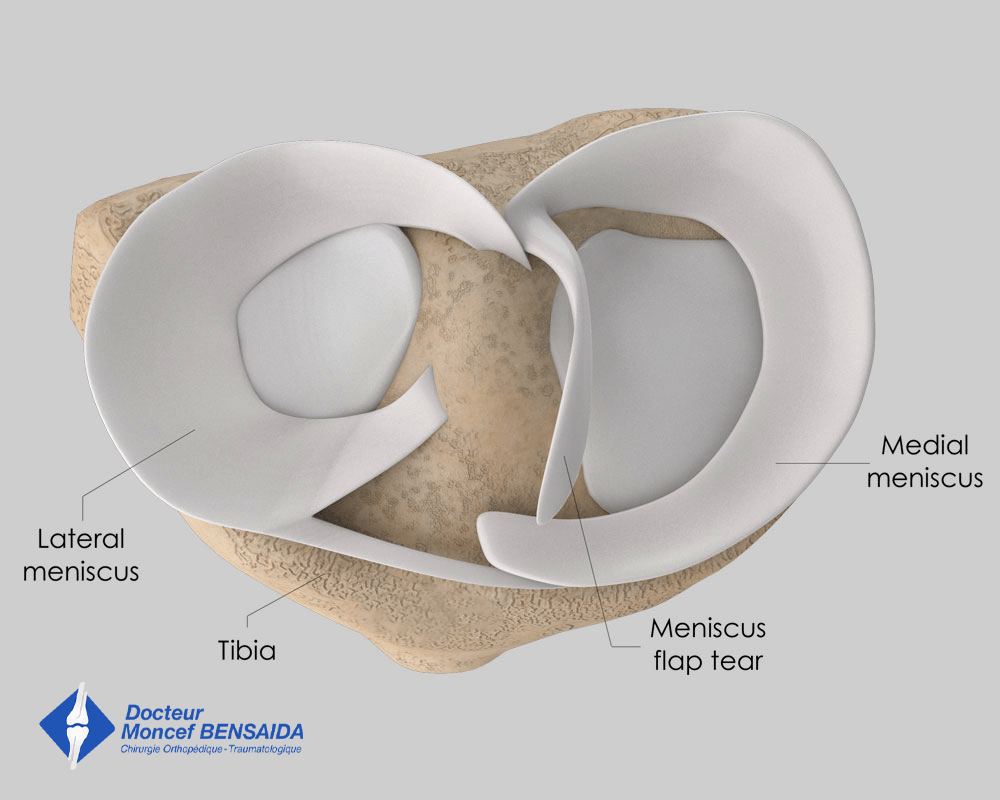
Unstable medial meniscal lesion with mobile flap
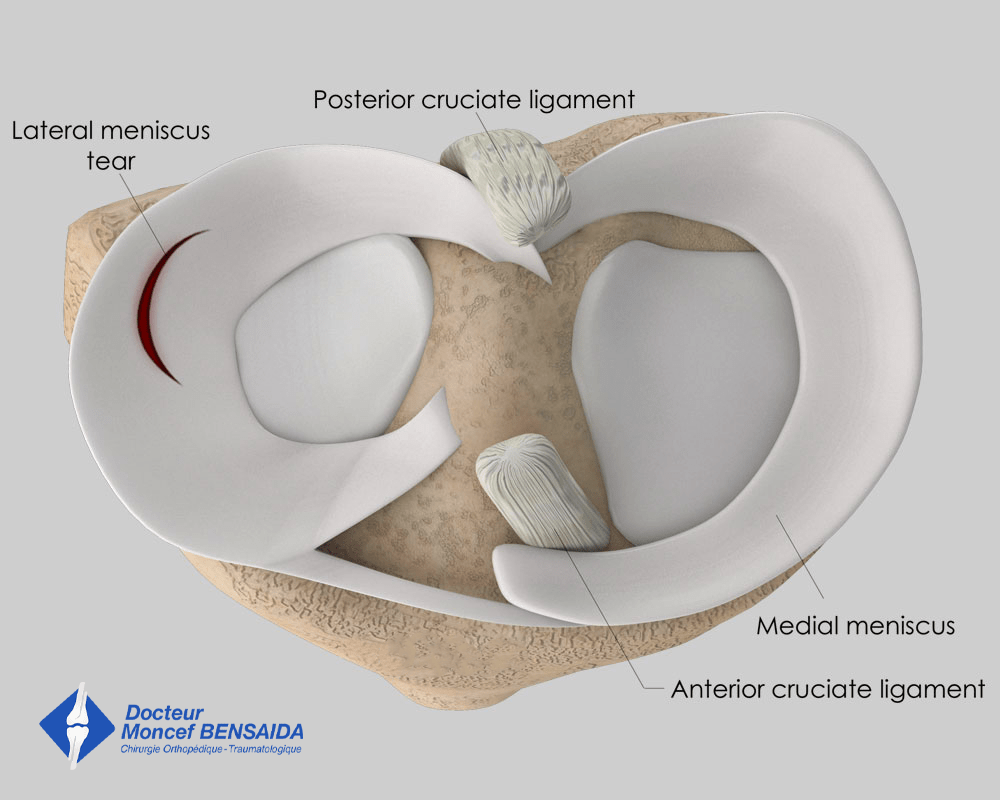
Stable lateral meniscal lesion
SYMPTOMS OF MENISCAL DAMAGE
Pain is the most common indicator associated with meniscal damage. It is generally located on either the medial or posterior side of the knee in the case of medial meniscal damage or conversely, on the lateral or posterior side of the knee in the case of lateral meniscal damage.
It usually occurs suddenly, immediately after the traumatising movement in the case of a traumatic injury.
However, pain linked to a degenerative meniscal lesion develops gradually and is not connected to a specific movement.
It is often felt in the days following an increase in physical effort, the day after a jog or long walk, for example.
This pain is often worse when crouching or going up or down stairs. It is often more intense at the end of the day and can sometimes persist into the night disrupting sleep. The knee may also be swollen.
Additionally, symptoms of an unstable meniscal lesion can include knee instability or locking associated with pain. During some movements, a mobile fragment can come between the femur and the tibia causing the knee to jerk and potentially give way. A “bucket handle” meniscal tear, so-called as it can flip over like a bucket handle, can block the knee. In this case, the knee is locked in bent position and the patient is unable to totally straighten it.
WHAT EXAMINATIONS ARE NECESSARY IN THE CASE OF A SUSPECTED MENISCAL LESION?
With a suspected meniscal lesion, two types of examinations are necessary. Firstly, knee x-rays are carried out to ensure there is no knee osteoarthritis. In the case of osteoarthritis, the pain is probably linked to the latter even if there is meniscal damage, which is often the case.
An MRI will also be carried out to examine the meniscal damage and determine its characteristics, especially whether it is stable or not. It will also highlight any related ligament damage.
In some cases, an MRI is contraindicated (patients with a Pace-Maker, presence of metal in the knee…). A CT arthrogram with the injection of an x-ray contrast medium in the joint is carried out instead and provides the same information as an MRI.
THE DIFFERENT THERAPEUTIC OPTIONS
The menisci protect the knee cartilage from wear (osteoarthritis). When possible, the various treatments aim to preserve the menisci as much as possible. There are three possible types of treatment:
- Medical treatment : analgesics and anti-inflammatories are combined to relieve the pain. If this is not enough, cortisone (a powerful anti-inflammatory) injected directly into the knee in contact with the damaged meniscus, can stop the pain. Finally, according to the shape of the patient’s knees and the meniscus involved, orthopaedic insoles can be prescribed which will modify weight-bearing and relieve the pain.
- A partial meniscectomy using arthroscopic surgery : this surgical treatment consists in removing the damaged part of the meniscus while sparing as much of the healthy part as possible. This procedure is performed arthroscopically requiring only 2 small incisions of a few millimetres on the anterior side of the knee. A camera and surgical instruments are inserted in the knee and the operation is monitored on a screen.
Unstable medial meniscal lesion with mobile flap
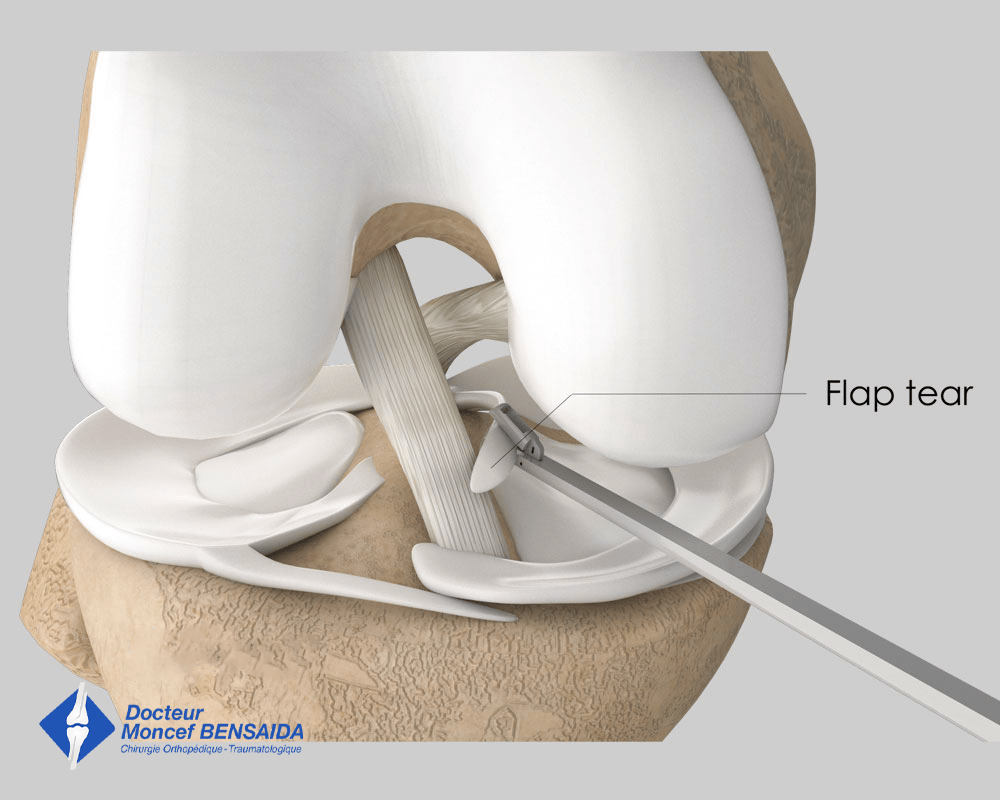
Partial medial meniscectomy
- Arthroscopic meniscal suture : when possible, this surgical treatment consists in repairing the meniscus by suturing the tear. In most cases, this procedure is carried out arthroscopically but may sometimes require an additional incision around the meniscal lesion to pass the sutures through. When an anterior cruciate ligament tear is also involved, the meniscal suture must be combined with anterior cruciate ligament reconstruction to have any chance of healing.

Suture of lateral meniscal lesion
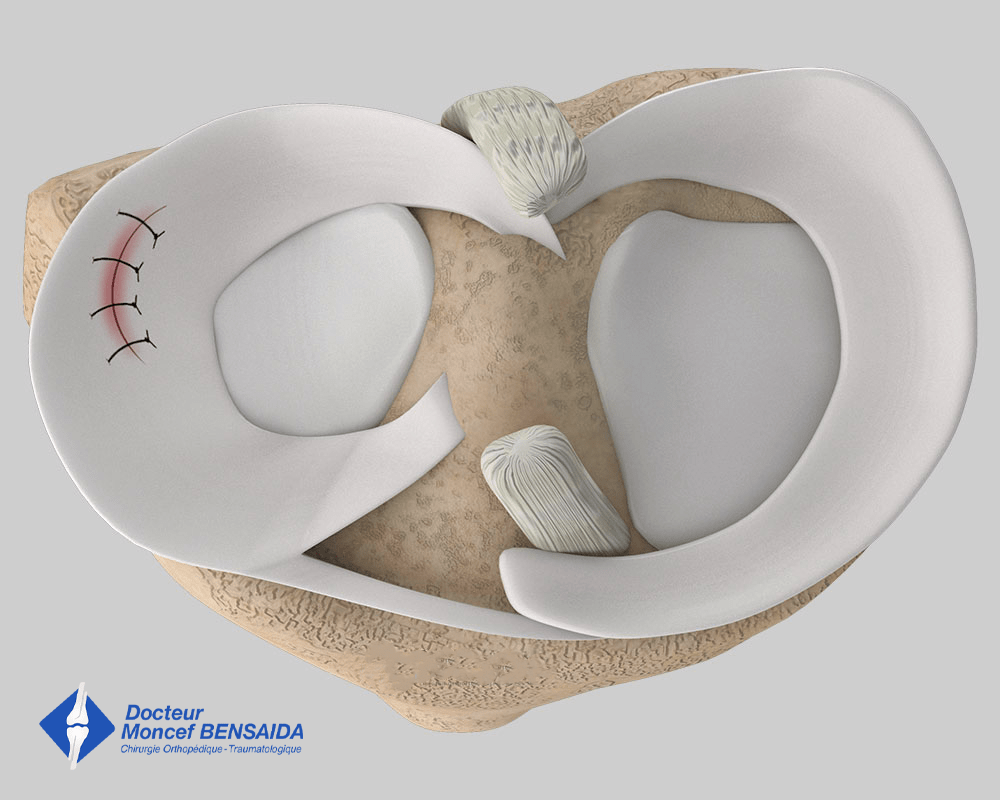
Final appearance of the lateral meniscal suture
WHICH TREATMENTS FOR WHICH PATIENTS?
IN YOUNG PATIENTS UNDER 40 YEARS
When possible, repairing the meniscus with sutures should be attempted. However, the possibility of repairing the tear depends on the location of the meniscal lesion and the condition of the meniscus. An MRI is carried out to determine if the meniscus can be repaired but this can only be assessed definitively during the operation.
If it is not possible to repair the meniscus and there is no mobile fragment in the knee, we will initially try to relieve the pain with a medical treatment. If this is unsuccessful, we will then proceed with a partial arthroscopic meniscectomy.
IN PATIENTS OVER 40 YEARS
Most lesions in patients over 40 years are the result of wear.
When the lesion is unstable with a mobile meniscal fragment, a partial meniscectomy will be carried out to remove the unstable fragment. This procedure aims to eliminate any instability and locking of the knee but may be partially effective or even ineffective on the pain.
When the lesion is stable, it is necessary to ensure that the meniscus is causing the pain, as degenerative meniscal lesions are often a result of knee ageing with osteoarthritis, which can also cause pain.
In the case of osteoarthritis, pain management involves treating the osteoarthritis and not the meniscal lesion.
In the absence of osteoarthritis, it is necessary to preserve the meniscus and relieve the pain with medical treatment. If the pain persists, a partial meniscectomy will be performed. In the case of degenerative damage, a meniscectomy sometimes only partially resolves the problem of pain and additional knee injections may be required.
MENISCAL SURGERY
This is an outpatient procedure (in one day). A pre-anaesthesia consultation is scheduled before the operation and a pre-operative assessment may be necessary to minimise the risk of complications. This operation can be carried out under general or spinal anaesthesia. The latter is a regional anaesthetic anaesthetising the lower part of the body (as with an epidural). The anaesthetist will decide on the most suitable anaesthetic together with the patient.
The operation takes place in an operating theatre in compliance with strict standards of cleanliness and safety. The patient is placed supine on an operating table and a tourniquet is placed around the top of the thigh.
The procedure lasts around thirty minutes plus the time required for the anaesthetic and preoperative preparations. In addition to the mensical surgery, the condition of the cartilage and the anterior cruciate ligament can be examined.
Immediately after the operation, the patient is taken to the recovery room to recover from the anaesthetic.
After the operation, the patient can put weight on the limb operated on. A slight limp is common in the first few days but crutches are rarely required.
Rehabilitation exercises are needed to recover knee mobility and are explained before leaving the clinic. If the patient does not feel they can do the exercises alone, rehabilitation sessions with a physiotherapist may be necessary.
In the case of meniscal repair, the knee can only be bent up to 90° for 6 weeks to avoid putting excessive strain on the sutures. Bending is not however restricted after a partial meniscectomy.
A postoperative check-up is scheduled 2 to 3 weeks after the operation to ensure good recovery, adjust rehabilitation, and identify any potential complications.
Sport can be resumed 6 weeks after the operation in the case of a meniscectomy and much later, in the 6th month, after meniscal repair.
From a practical point of view, medical leave varies according to the procedure carried out (repair or meniscectomy) as well as the nature of the patient’s profession (physical or sedentary) but generally varies from 10 days to 1 month. It is possible to start driving again in the week following the operation, as soon as the patient is capable of doing an emergency stop.
RISKS LINKED TO THE OPERATION
Unfortunately, zero risk does not exist in surgery. Any operation has its risks and limitations, which you must accept or not undergo the operation. However, if an operation is proposed, the surgeon and the anaesthetist consider that the expected benefits far outweigh the risk incurred.
Some risks, such as microbial infections of the surgical site, are common to all types of surgery. Fortunately, this complication is rare but when it occurs requires another operation and a course of antibiotics. Bruising can also appear around the surgical site. This is usually avoided or reduced with a suction drain inserted at the end of the operation and removed in the days following the operation.
Knee surgery also increases the risk of phlebitis, which can lead to a pulmonary embolism. To minimise this risk, blood thinners (in the form of daily injections) are prescribed for 1 week following the operation.
In rare cases, the knee remains stiff, hot, and painful for several months after the operation. This complication, known as algodystrophy or Chronic Regional Pain Syndrome (CRPS), is unpredictable and sometimes takes a long time to heal.
Nerves can also be damaged accidentally during the operation with a risk of paralysis or loss of feeling in the limb operated on, which can be transitory or permanent.
If you have any concerns about the operation, do not hesitate to talk to your surgeon or the anaesthetist and they will answer any questions you may have.