ORIGIN AND NATURAL HISTORY OF CALCIUM DEPOSITS
ORIGIN AND NATURAL HISTORY OF CALCIUM DEPOSITS
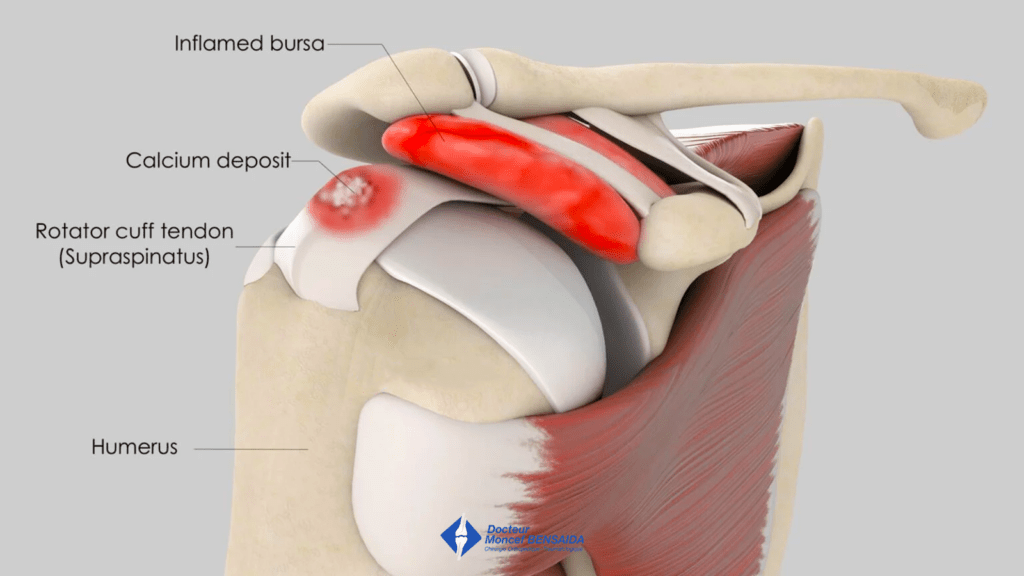
The rotator cuff is a group of four muscles located in the shoulder involved in lateral elevation and rotation of the arm. These muscles are attached to the humerus with tendons in which one or several calcium deposits can be found. This is known as calcific tendonitis of the rotator cuff.
Calcific tendonitis is a common pathology affecting approximately 5% of the general population but the origin of the calcium deposits is unknown. It has been suggested that it is caused by the abnormal healing of the tendon damaged as a result of microtrauma but the fact that the dominant side is not involved more goes against a mechanical cause. It is actually the spontaneous transformation of the tendon structure and genetic causes that are today being suggested.
The calcium deposits generally progress in 3 phases.
Formative phase
The structure of the tendon changes around a calcium deposit giving rise to a calcification that continues to increase in size until it stabilises. This phase is generally asymptomatic.
Calcific phase (= chronic phase)
The calcium deposit is very hard during this phase and the tendon pain often experienced is linked to the hyper-pressure created by the calcium deposit inside the tendon. Due to its increase in size, the tendon can also catch on the acromion, the bony arch overhanging the rotator cuff tendons, when moving the arm. This is known as sub-acromial impingement.
Resorption phase
During the resorption phase, the hard calcium deposit softens. The volume and tension of the calcium deposit increase, signs of inflammation appear and the pain is caused mainly by the inflammation of the subacromial bursa due to the calcium microcrystals released. During this phase, the pain is intense, causing insomnia and it is impossible to actively move the arm.
At the end of this phase, the tendon heals and recovers normally.
CLASSIFICATION OF CALCIUM DEPOSITS
The radiographic morphology of the calcium deposits is the best indication of the stage.
It is dense and the edges are sharp in the formative and chronic phases.
In the resorption phase, the calcium deposits firstly become more translucent then the edges become blurred and heterogeneous.
Classification type A
Dense, homogeneous, round with a sharp outline

Classification type B
Dense, homogeneous, multilobular with a sharp outline

Classification type C
Cloudy, heterogeneous with a blurred outline
Transitory-C: progression towards spontaneous resorption (a new x-ray a few months later will show the calcium deposit has been totally resorbed)
Persistent-C: progression stops; the x-ray does not change

WHAT IS THE PROBLEM?
Generally, small calcium deposits are asymptomatic and only the largest ones are painful.
A calcium deposit naturally progresses through different stages until it is spontaneously resorbed. Healing can cause episodes of pain, sometimes intense.
The calcium deposit and symptoms can take a few months to several years to disappear. It is unpredictable.
Sometimes, the progression stops at the calcific phase (persistent type A or B) or the resorptive phase (persistent type C) and the pain persists.
WHAT EXAMINATIONS ARE NECESSARY?
X-rays are best to assess calcific tendonitis of the rotator cuff. The calcification can be located and the phase determined. In 80% of cases, it involves the supraspinatus tendon, in 15% of cases the infraspinatus tendon, and in 5% of cases the subscapularis tendon.
An MRI is sometimes requested to identify any potential tears involving the rotator cuff tendons.
WHAT TREATMENTS ARE AVAILABLE?
Medicinal treatments
Corticosteroid injections
X-ray-guided corticosteroid injections in the subacromial space can have beneficial effects, especially in the resorptive phase (type C) when there is significant inflammation of the subacromial bursa.
Extracorporeal shock waves
These are acoustic waves, ideally high energy focused, delivered by a machine on the surface of the skin above the diseased tendon the aim of which is to loosen the calcium fixed to the tendon to eliminate it.
Shock waves are preferably indicated in the calcific stage when the calcium deposit is hard. Three sessions are recommended and the efficacy of this treatment varies from 10 to 70% depending on the studies.
Lavage-Aspiration
The lavage and aspiration are ultrasound or x-ray-guided. This treatment is often combined with corticosteroid injections in the calcium deposit and is only possible once the calcium deposit has softened (type C).
Surgical treatment
Arthroscopic surgical treatment consists in removing the calcification and potentially giving the tendon more space by increasing the subacromial space. This is achieved with an acromioplasty.
WHEN IS SURGERY NECESSARY?
If the medical treatment does not relieve the pain, surgical treatment can be proposed.
It is necessary to ensure beforehand that the calcification is not spontaneously resorbing, which can trigger or increase the pain and lead the patient to consult a surgeon. In this situation, surgery would be pointless and it is therefore important to carry out 2 x-rays at least 3 months apart showing no change in the appearance of the calcification.
Finally, before operating, it is necessary to ensure that the shoulder is not stiff, as this would indicate adhesive capsulitis secondary to the calcific tendonitis for which surgery is contraindicated. In this case, rehabilitation is preferred with balneotherapy to recover joint range of motion.
THE OPERATION
The operation is planned during pre-surgical consultations. A pre-anaesthesia consultation before the operation, and possibly a pre-operative assessment, is conducted to minimise the risk of complications. This procedure is usually carried out under general anaesthesia. The anaesthetist will decide on the most suitable anaesthetic together with the patient.
The operation lasts about 45 minutes.
The operation takes place in an operating theatre in compliance with strict standards of cleanliness and safety. The patient is put in the beach chair or lateral decubitus position, and mild traction is applied to the arm.
Arthroscopy
The procedure is carried out arthroscopically, a minimally invasive surgical technique. Very small incisions of a few millimetres are made in the skin through which a camera and the instruments required for the operation can be inserted in the shoulder. Arthroscopic surgery enables the damage to be assessed and the scheduled procedures to be performed while minimising the trauma for the shoulder and the unsightly appearance (small scars).
What procedures are carried out?
Subacromial bursectomy
This is the first stage of the operation and involves removing the subacromial bursa that contains calcium microcrystals, which is often very inflamed and painful as a result.
Location and removal of the calcification
As the calcification is inside the tendon, it is not visible and must be located. If it is very large, it can be easily located as it deforms the tendon. In other cases, the tendon is not deformed and is explored with a hollow needle. The location of the calcification is confirmed by the obstruction of the needle point with a calcium deposit and/or calcium fragments where the tendon was perforated with the needle.
Once the calcification is located, the tendon is cut lengthwise to remove the calcification, which is aspirated using specific instruments. Once removed, the tendon is left as it is and heals spontaneously.
In rare cases, especially with type C calcification, the calcification is not located and an acromioplasty is thus performed.
Acromioplasty
This involves thinning the acromion, the bone under which the damaged tendon(s) slide. An acromioplasty is not systematically carried out. It is performed in the case of type C calcification, failure to remove the calcium deposit or pathological aspect of the superficial side of the rotator cuff tendon(s).
Rotator cuff repair
During an operation, it is rare to discover a rotator cuff tendon tear where the calcification is located but if this is the case, the tendon is repaired.
AFTER THE OPERATION
Postoperative pain is managed by the anaesthetists who often use an interscalene nerve block that numbs the shoulder and the upper limb for several hours after the patient wakes up.
The shoulder does not need to be immobilised but the arm will be placed in a sling for the first few days to limit postoperative pain.
The patient can return home the same day (outpatient surgery) or the day after the operation.
Mobilisation should begin early. Self-rehabilitation exercises will be explained by the physiotherapists during your stay at the clinic and more intensive rehabilitation will begin with a local physiotherapist. Rehabilitation often lasts between 1 and 2 months.
Follow-up consultations are scheduled 1 and 3 months after the operation to ensure good recovery and adjust rehabilitation, as well as to detect any potential complications. During these consultations, the progressive disappearance of the calcification is verified on x-rays.
It generally takes 3 to 6 months for the pain to totally disappear.
From a practical point of view, medical leave is often between 3 and 6 weeks but depends on the patient’s profession and the side operated on (dominant or not). Driving can be resumed around 3 weeks after the operation and sports activities can be resumed from the 3rd month after the operation.
RISKS LINKED TO THE OPERATION
Unfortunately, zero risk does not exist in surgery. Any operation has its risks and limitations, which you must accept or not undergo the operation. However, if an operation is proposed, the surgeon and the anaesthetist consider that the expected benefits far outweigh the risk incurred.
Some risks, such as microbial infections of the surgical site, are common to all types of surgery. Fortunately, this complication is rare but when it occurs requires another operation and a course of antibiotics. Bruising can also appear around the surgical site.
In rare cases, the shoulder may remain stiff and painful for several months after the operation. This complication, known as capsulitis, is linked to the unpredictable reaction of the sympathetic nervous system and takes a long time heal.
Nerves can also be damaged accidentally during the operation with a risk of paralysis or loss of feeling in the limb operated on, which can be transitory or permanent.
If you have any concerns about the operation, do not hesitate to talk to your surgeon or the anaesthetist and they will answer any questions you may have.