ARTHROSCOPIC ROTATOR CUFF REPAIR
WHAT IS THE PROBLEM?
The rotator cuff is a group of four muscles located in the shoulder involved in lateral elevation and rotation of the arm. These muscles are attached to the humerus with tendons that can tear progressively due to ageing or suddenly as a result of trauma.
Progressive tears, known as degenerative, generally occur after the age of 50. They often cause pain but minimal loss of mobility. The progressive nature of the tears enables the other muscles to develop to offset the deficit linked to the torn tendon(s).
Traumatic tears occur more often after the age of 40 following a fall or shoulder dislocation resulting in pain and a significant decrease in shoulder mobility, as the brutal nature of the tear does not allow the other muscles to compensate.
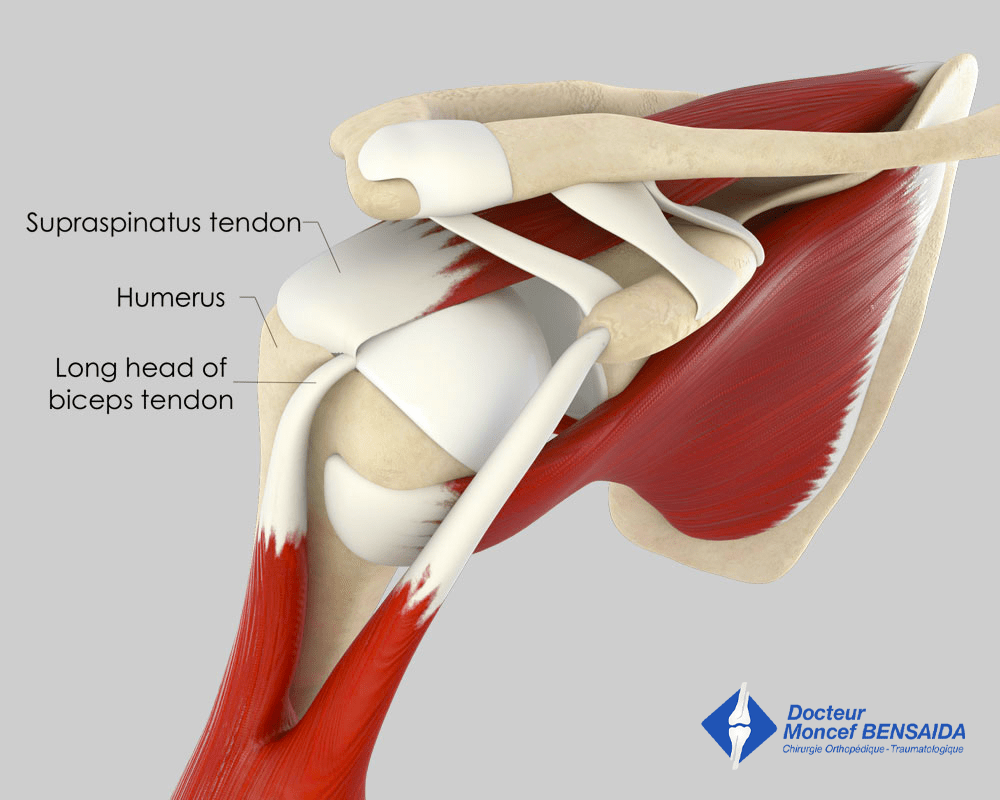
Normal shoulder (anterior view)
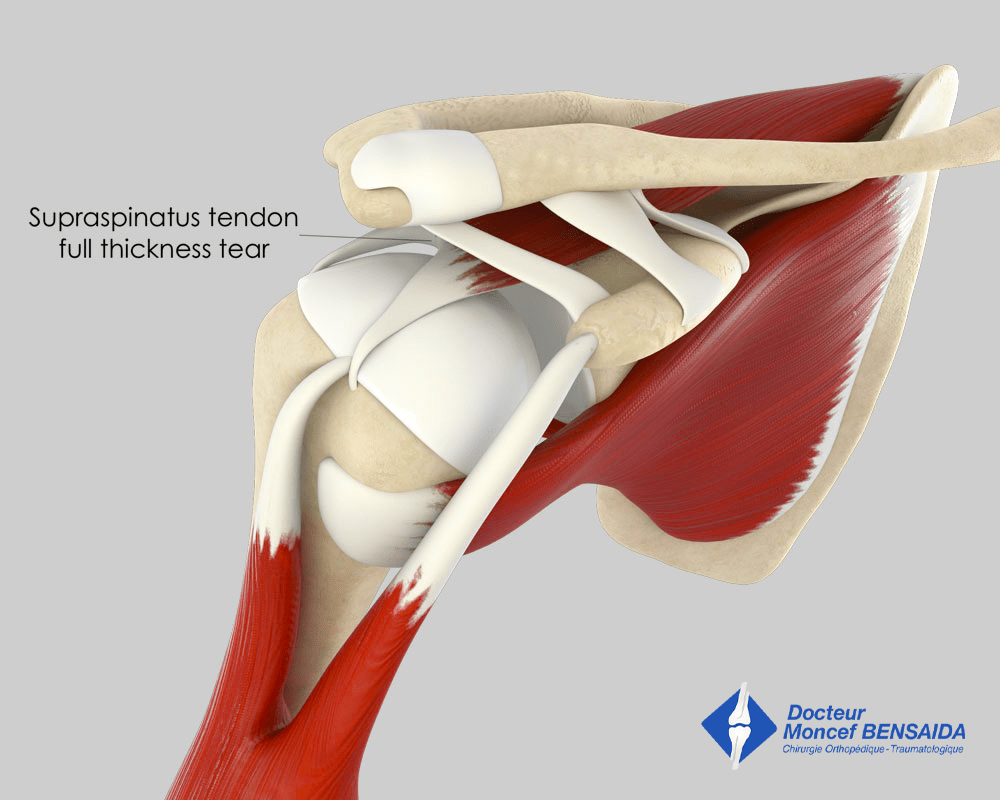
Rotator cuff tendon tear
WHAT EXAMINATIONS ARE NECESSARY?
If a rotator cuff tear is suspected during a consultation, shoulder x-rays and an ultrasound scan must be performed. If the ultrasound scan confirms the tear and surgical repair of the rotator cuff is considered, an MRI or CT arthrogram (a contrast medium is injected in the joint) must be carried out. This examination aims to assess whether the rotator cuff tear can be repaired or not.
WHAT ARE THE PROSPECTS WITH A TORN ROTATOR CUFF?
Traumatic rotator cuff tears are often badly tolerated and surgery is necessary. Degenerative tears that appear more gradually can be tolerated from a functional point of view and possibly improved with rehabilitation and shoulder injections but with some loss of strength and sometimes range of motion.
However, massive rotator cuff tears involving several rotator cuff tendons can lead to shoulder cartilage wear, known as omarthrosis, which may ultimately require a shoulder replacement.
WHEN IS IT NECESSARY TO OPERATE ON ROTATOR CUFF TEARS?
An operation is never systematic and depends on the nature of the rotator cuff tear and its tolerance from a functional point of view.
Traumatic ruptures are often badly tolerated and require an operation.
Degenerative tears must initially be treated with a combination of medical treatment including shoulder injections and rehabilitation sessions. When this treatment is no longer enough to relieve the patient, surgery may be considered.
THE OPERATION
The procedure is planned during pre-surgical consultations. A pre-anaesthesia consultation before the operation and a pre-operative assessment are conducted to minimise the risk of complications. This procedure is usually carried out under general anaesthesia. The anaesthetist will decide on the most suitable anaesthetic together with the patient.
The operation takes place in an operating theatre in compliance with strict standards of cleanliness and safety, and lasts about 1 hour. The patient is put in the beach chair or lateral decubitus position, and mild traction is applied to the arm.
Arthroscopy
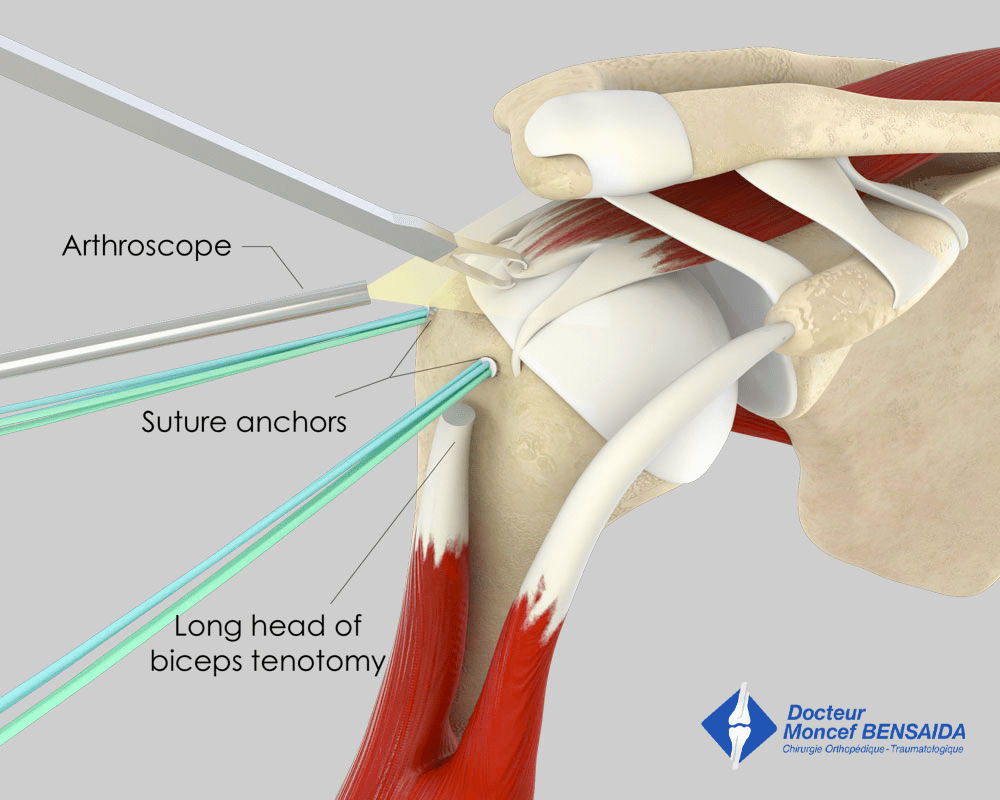
Procedures on the rotator cuff are performed arthroscopically, a minimally invasive surgical technique. Very small incisions of a few millimetres are made in the skin through which a camera and the instruments required for the operation can be inserted in the joint. Arthroscopic surgery enables the damage to be assessed and the scheduled procedures to be performed while minimising the trauma for the shoulder and the unsightly appearance.
In rare cases, open surgery with a larger incision is necessary.
What procedures are carried out?
Different surgical procedures can be performed and potentially combined during the operation :
- Rotator cuff tendon repair : consists in reinserting the torn tendons in their usual attachment site using anchors. Only repairing the tendons is likely to restore shoulder strength and unfortunately, this is not always possible, especially for old tears where the muscle has totally atrophied and the tendon retracted and can no longer reach its insertion site.
- Tenotomy of the long head of the biceps tendon : consists in cutting one of the two tendons attaching the biceps muscle to the shoulder. This procedure is very effective in decreasing shoulder pain, as the cut tendon is often diseased and very inflamed when there is a rotator cuff tear. This tenotomy leads to a decrease in biceps muscle strength of only 6%, which is generally imperceptible for the patient. However, in some thin subjects, the tenotomy results in a Popeye deformity visible when contracting the muscle and has functional consequences. The long biceps tendon can be attached a little lower to the arm bone. This is known as a tenodesis and reduces the risk of a Popeye deformity in thin subjects and the loss of strength for manual workers doing repetitive movements. The risk of residual pain is however greater after a tenodesis than after a tenotomy.
- Acromioplasty : involves removing the sharp bone spur called acromial spur located under the arch where some of the rotator cuff tendons are located. The contact between the acromial spur and the rotator cuff tendons often causes the impingement that resulted in the tendon tear.
- Subacromial bursectomy : consists in removing the tissue located on the rotator cuff, known as the subacromial bursa. This tissue is often very inflamed with rotator cuff tears and its removal helps decrease the pain.
- Resection of the acromioclavicular joint : consists in decreasing the rubbing between the clavicle and the shoulder blade, which is sometimes diseased and painful and contributes to the development of the acromial spur.
Rotator cuff repair
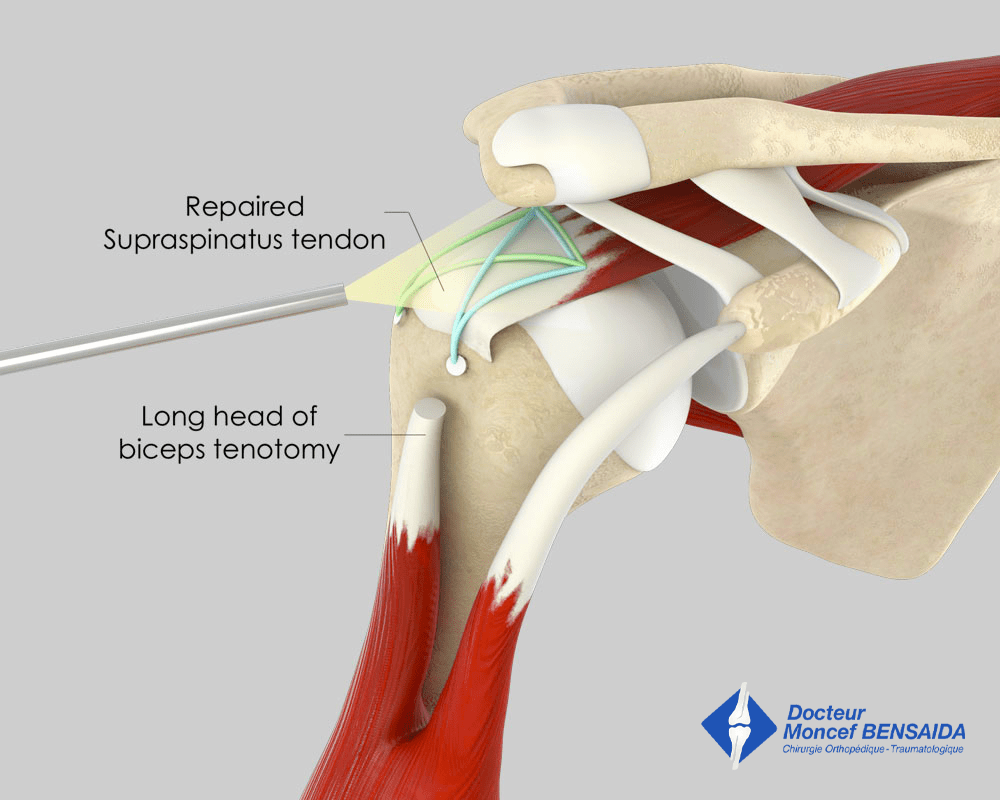
Final appearance of the repair
L'INTERVENTION
Arthroscopic rotator cuff repair is a surgical procedure used to treat rotator cuff injuries of the shoulder. It is performed using an arthroscope, a thin instrument with a camera, which is inserted into the shoulder through small incisions. This technique allows the surgeon to view the inside of the shoulder joint without needing to make a large incision.
During the procedure, the surgeon uses special instruments to repair damaged rotator cuff tendons. This may involve suturing torn tendons, removing degenerated tissue, or removing bone spurs that are contributing to subacromial impingement. The repair aims to restore rotator cuff functionality, reduce pain, and improve shoulder mobility.
After surgery, the patient may complete a rehabilitation program supervised by a physical therapist to strengthen the shoulder muscles, improve stability, and regain full range of motion. Recovery time may vary depending on the severity of the injury and the patient’s individual response to rehabilitation, but it may take several months before the shoulder returns to optimal strength and functionality.
AFTER THE OPERATION
Postoperative pain is managed by the anaesthetists who often use an interscalene nerve block that numbs the shoulder and the upper limb for several hours after the patient wakes up.
The patient can return home the day of the operation or the day after.
After the operation, a shoulder immobilisation brace must be worn and this for 6 weeks in the case of rotator cuff repair. It can be removed for a few hours a day but your arm must be kept straight against the side of your body.
Self-rehabilitation exercises will be explained by the physiotherapists during your stay at the clinic and must be done throughout the first 6 weeks after the operation.
Subsequently, more intensive rehabilitation with a local physiotherapist will begin. Rehabilitation often lasts between 3 and 6 months.
Follow-up consultations will take place 1, 3, and 6 months after the operation to ensure good recovery and adjust rehabilitation as well as to detect any potential complications.
From a practical point of view, medical leave is between 6 weeks and 6 months but depends on the patient’s profession and the side operated on (dominant or not). Car driving can be resumed around the 2nd month after the operation.
HOW LONG DOES IT TAKE TO RECOVER AFTER THE OPERATION?
Recovery from rotator cuff repair is often long and it is not uncommon that it requires 6 months.
The tendons can tear again with time. Nevertheless, these iterative tears are often not as extensive as the initial tears and tolerated better.
RISKS LINKED TO THE OPERATION
Unfortunately, zero risk does not exist in surgery. Any operation has its risks and limitations, which you must accept or not undergo the operation. However, if an operation is proposed, the surgeon and the anaesthetist consider that the expected benefits far outweigh the risk incurred.
Some risks, such as microbial infections of the surgical site, are common to all types of surgery. Fortunately, this complication is rare but when it occurs requires another operation and a course of antibiotics. Bruising can also appear around the surgical site.
In rare cases, the shoulder may remain stiff and painful for several months after the operation. This complication, known as capsulitis, is linked to the unpredictable reaction of the sympathetic nervous system and can take a long time to heal.
Nerves can also be damaged accidentally during the operation with a risk of paralysis or loss of feeling in the limb operated on, which can be transitory or permanent.
If you have any concerns about the operation, do not hesitate to talk to your surgeon or the anaesthetist and they will answer any questions you may have.