POSTERIOR CRUCIATE LIGAMENT RECONSTRUCTION
Posterior Cruciate Ligament Surgery, also known as PCL reconstruction, is a specialized orthopedic surgical procedure to restore stability to the knee in cases of injury or tear to the posterior cruciate ligament.
Why is PCL Ligamentoplasty necessary?
The posterior cruciate ligament (PCL) plays a crucial role in knee stability by preventing the lower leg from sliding backward relative to the thigh. An injury to the PCL can occur following a sports trauma, a road accident or a significant fall. Without proper treatment, this can lead to knee instability, persistent pain, and decreased mobility.
The PCL Ligamentoplasty Process
During PCL ligamentoplasty, the specialized orthopedic surgeon performs reconstruction of the damaged ligament using autologous grafts (from the patient’s own) or allogeneic grafts (from a donor). The technique chosen will depend on the patient’s individual situation.
The Advantages of PCL Ligamentoplasty
- Recovered Stability : PCL ligament reconstruction helps restore knee stability, which is essential for returning to normal activities.
- Pain Reduction : This procedure can help reduce pain and improve the patient’s quality of life.
- Return to Activity : With appropriate rehabilitation, many patients can return to their previous level of activity, including sports activities.
The choice of PCL ligamentoplasty technique and the success of the procedure will depend on the specific needs of each patient. An experienced orthopedic surgeon can assess the situation and recommend the most appropriate treatment plan.
If you suffer from a PCL injury or have any questions about PCL ligamentoplasty, do not hesitate to make an appointment for a consultation. We are here to offer you specialized and personalized orthopedic care.
WHAT IS THE PROBLEM?
Under normal conditions, the knee is a stable joint and so dislocation is extremely rare. Anatomical components called ligaments ensure knee stability. Ligaments are like relatively inelastic ropes connecting the different bones in the knee.
The posterior cruciate ligament (PCL) is a ligament located in the middle of the knee between the femur and the tibia. It participates in knee stabilisation by preventing the tibia from moving too far backwards.
Posterior cruciate ligament rupture can be caused by an impact to the front of the leg, which generally occurs during a road accident or more rarely a sports trauma.
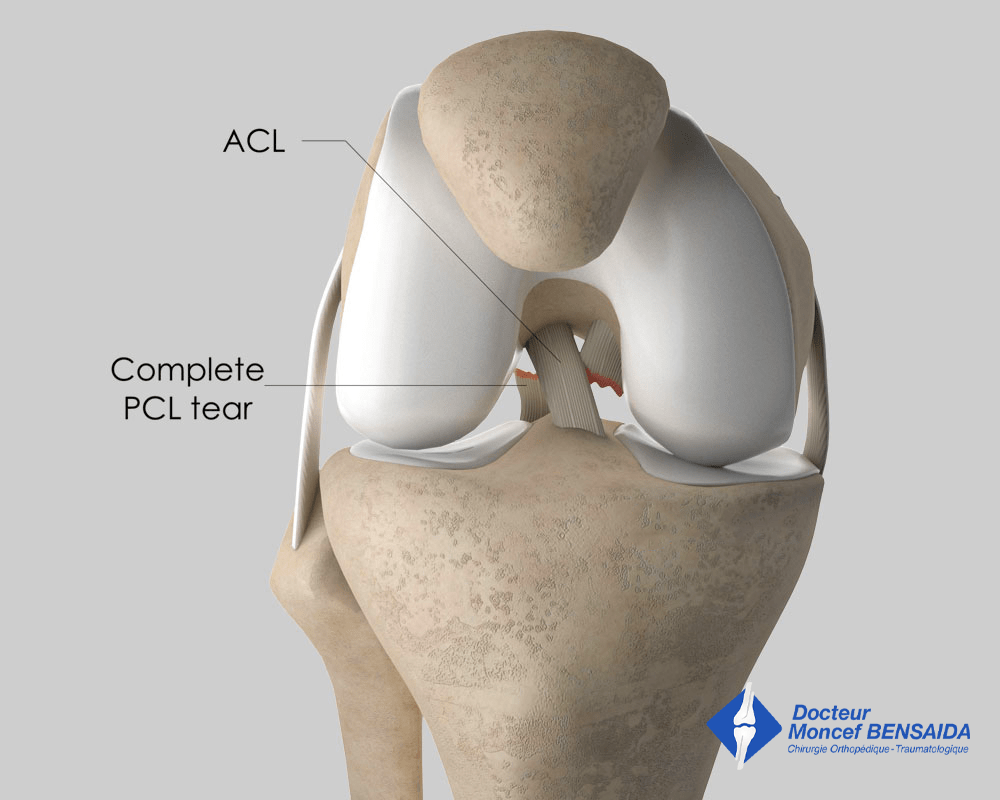
Posterior cruciate ligament rupture (anterior view)
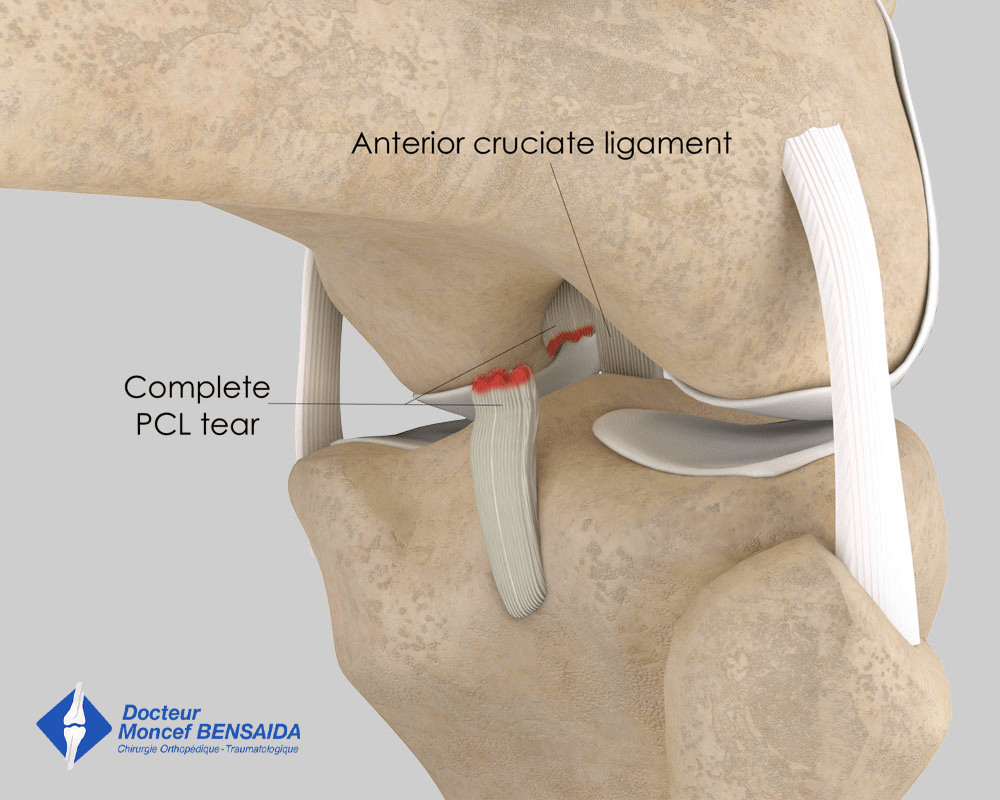
Posterior cruciate ligament rupture (posterior view)
Ultimately, the consequences of posterior cruciate ligament rupture vary from one patient to another but it primarily develops in the following ways:
- The patient does not complain. The knee remains stable and painless after rehabilitation. This is the most common course when only the PCL is torn.
- The patient develops patellar pain caused by posterior translation of the tibia called posterior drawer due to PCL rupture. This leads to an increase in pressure on the patella, especially when sitting or going down stairs.
- The patient develops knee instability. This instability is much rarer than in the case of anterior cruciate ligament rupture.
WHAT EXAMINATIONS ARE NECESSARY?
Immediately after the sprain, knee x-rays need to be performed to rule out a joint fracture of which the initial symptoms are very similar to a posterior cruciate ligament tear.
Once a fracture is ruled out, the patient must be examined by a doctor. A clinical examination immediately after a knee sprain is difficult due to the pain and often requires a reassessment two weeks later once the swelling has gone down and the pain receded. Most often, a clinical examination is sufficient to diagnose a posterior cruciate ligament tear. However, it is customary to perform a Magnetic Resonance Imaging (MRI) scan to confirm posterior cruciate ligament damage and highlight any other potential damage, especially to the peripheral ligaments and the menisci.
The surgeon can also request other x-rays of the knee to assess any cartilage wear, which can modify the indication or the type of operation proposed.
Finally, the surgeon may request dynamic x-rays (TELOS) to assess posterior knee laxity caused by posterior cruciate ligament rupture.
WHAT TREATMENTS ARE AVAILABLE?
Non-surgical treatment
This is indicated in the acute phase of the sprain if only the PCL is involved and posterior laxity due to the ligament tear is minor. It combines initial pain-killing measures (ice, analgesics, anti-inflammatories) and immobilisation of the knee in extension in an appropriate brace for 6 weeks.
Resumption of weight-bearing is progressive according to the pain and rehabilitation focuses on strengthening the quadriceps.
Surgical treatment
Contrary to anterior cruciate ligament tears, there is no formal consensus regarding the repair of PCL tears. However, some trends have emerged over the past decade.
→Acute phase
In the early stages, surgery on the PCL is necessary when associated with a peripheral knee ligament tear. These are serious combined injuries of which the progression in the absence of surgery is unfavourable from a functional point of view.
Corrective surgery can also be proposed when only the PCL is involved but causing severe posterior knee laxity in young, athletic patients.
→Chronic phase
With old PCL tears, an operation is required in the event of knee instability or patellar pain linked to the posterior drawer.
The operation proposed
The surgery depends on how old the PCL lesion is.
→Recent PCL lesions:
When the lesion is recent (< 1 month), the PCL has the potential to heal and the surgery consists in positioning a brace along the damaged ligament to reduce posterior drawer in the knee and allow the PCL to heal. This brace can be biological (1 or several tendons are taken from the same knee) or synthetic. The advantage of a synthetic ligament is that no tendon needs to be harvested from the knee operated on.
→Old PCL lesions:
In the chronic phase, one or several tendons harvested from the same knee are used to reconstruct the PCL. For example:
- tendons of the gracilis and semitendinosus muscles
- part of the quadriceps tendon
- part of the patellar tendon
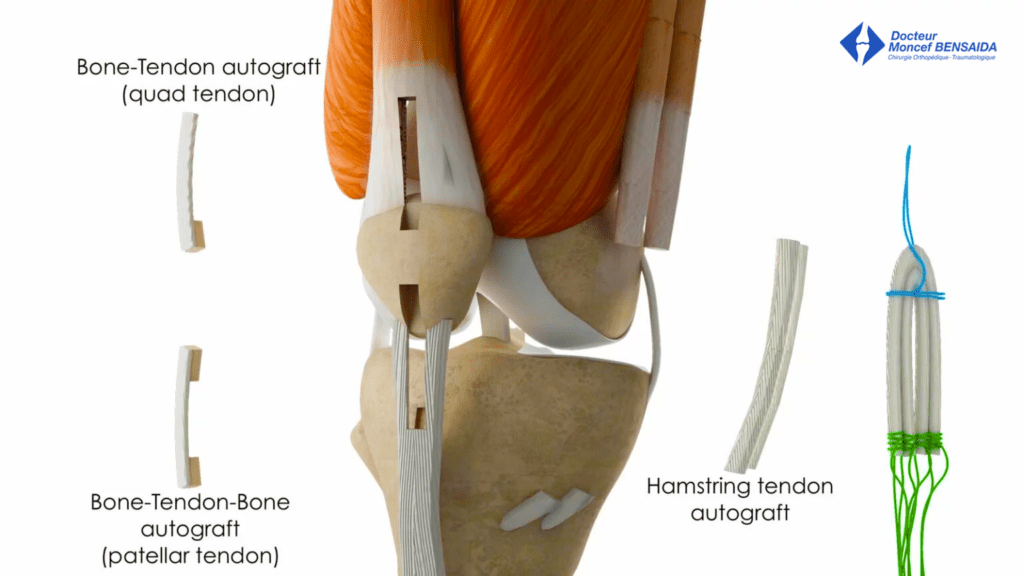
Tendons used as grafts to reconstruct the PCL
THE OPERATION
If surgery is scheduled, the patient must consult an anaesthetist to determine the most appropriate anaesthesia with regard to the patient’s state of health. The anaesthesia will be either general (patient unconscious) or regional (spinal block) where only the lower part of the body is anaesthetised.
The operation takes place in an operating theatre in compliance with strict standards of cleanliness and safety. The patient is placed supine on an operating table and a tourniquet is placed around the thigh.
The main procedure: posterior cruciate ligament reconstruction
Unless a synthetic artificial ligament is used, the first stage of the operation involves harvesting the tendon(s) that will be used as a graft to reconstruct the PCL.
In the case of reconstruction using the tendons of the gracilis and semitendinosus muscles, the tendons are harvested through a short incision of 2 centimetres on the anterolateral side of the leg, 5 centimetres below the knee.
An incision is made 5 centimetres above the patella if part of the quadriceps tendon is used and 5 centimetres below the patella if the patellar tendon is used.
The next step is performed using arthroscopic surgery, a minimally invasive surgical technique that enables the operation to be carried out through two small incisions 5 millimetres in length located on the anterior side of the knee. A miniaturised camera is inserted in the joint so the procedure can be followed on a screen. The graft or synthetic tendon is inserted in the joint where it is fixed in the bone tunnels created by the surgeon in the posterior cruciate ligament insertion sites on the femur and tibia.
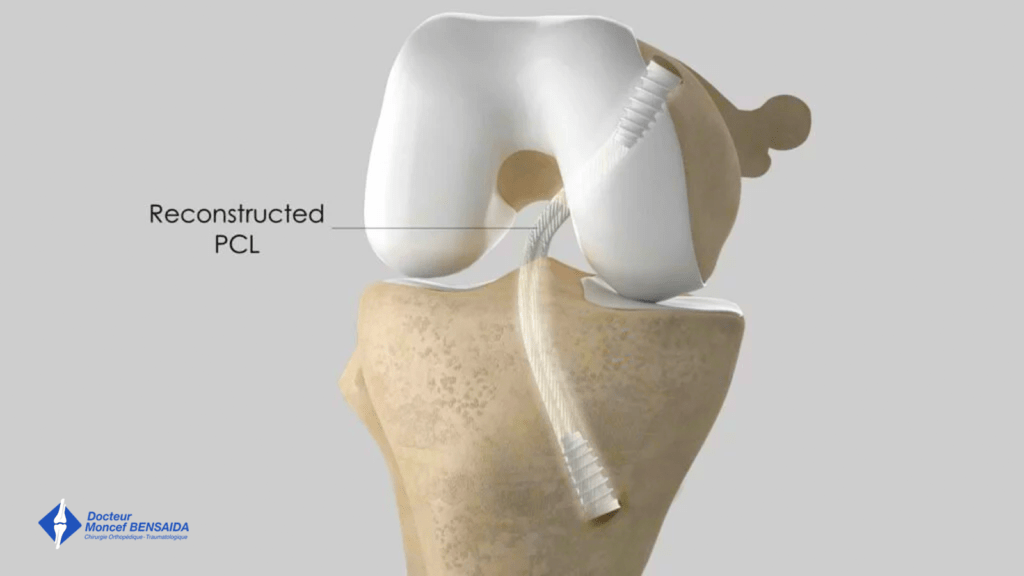
PCL reconstruction: final appearance with graft fixed in place using interference screws
Additional procedures
Any peripheral ligament damage will be repaired during the operation. The peripheral ligaments are located outside the joint. Consequently, an incision in the skin is required to repair the damaged structures.
Finally, any meniscal damage can be treated during the operation. The meniscus is repaired or the damaged part removed.
Before closing up, a drain (Redon) is often inserted in the incision to drain the blood and prevent the formation of a haematoma. This drain is generally removed just before the patient is discharged.
In general, the procedure lasts between 1 hour and 1 hour 30 minutes.
No blood transfusion is necessary for this operation.
AFTER THE OPERATION
The initial pain is usually managed well with drugs or even a nerve block (placed in the operating theatre by the anaesthetist), which keeps the knee numb for several hours after the operation.
A short stay of fewer than 2 days is usually required for this operation.
Weight-bearing is allowed from the outset but must be aided with crutches for 3 weeks. An articulated knee brace is used for 6 weeks to restrict posterior translation of the tibia.
During the first month after the operation, you must reduce your level of activity. A nurse will visit you at home for the first three weeks to change the dressings and administer the anticoagulant injections.
Rehabilitation begins early in the days following the operation. The initial aim is to wake up the muscles, help the swelling of the knee go down, and recover flexibility.
A check-up is scheduled one month after the procedure to assess recovery and progress made, as well as to adjust rehabilitation if progress is not as expected. Other check-ups are usually scheduled during the 3rd and 6th month after the operation.
You must remember that it is normal for your knee to remain swollen in the weeks following the operation. The pain will gradually fade over time and you will usually recover good knee function for daily life 6 weeks after the operation. However, this is an average and may take longer for some patients.
RESUMING WORK AND SPORT
The duration of medical leave depends on the patient’s profession and the type of operation but is usually between 1 and 3 months.
Sport can be resumed progressively. An exercise bike can be used soon after the operation. Running on flat ground (athletics track or treadmill) can be resumed from the 4th month and on any ground from the 6th month. Swimming with a flutter kick can also be resumed from the 3rd month. Most sports can be resumed from the 6th month; however, particular caution must be taken with pivoting sports (football, ski, judo) for which it is necessary to wait until the 9th month.
The return to sport may differ depending on the additional procedures performed on the meniscus or cartilage.
RISKS LINKED TO THE OPERATION
Unfortunately, zero risk does not exist in surgery. Any operation has its risks and limitations, which you must accept or not undergo the operation. However, if an operation is proposed, the surgeon and the anaesthetist consider that the expected benefits clearly outweigh the risk incurred.
Some risks, such as microbial infections of the surgical site, are common to all types of surgery. Fortunately, this complication is rare but when it occurs requires another operation and a course of antibiotics. Bruising can also appear around the surgical site. This is usually prevented or reduced with a suction drain inserted at the end of the operation and removed in the days following the operation.
Knee surgery also increases the risk of phlebitis, which can lead to a pulmonary embolism. To minimise this risk, blood thinners (in the form of daily injections) are prescribed for 3 weeks following the operation.
In rare cases, the knee remains stiff, hot, and painful for several months after the operation. This complication, called algodystrophy or Chronic Regional Pain Syndrome (CRPS), is unpredictable and sometimes takes a long time to heal.
Quite often, a small area of skin around the incision made to harvest the tendon or a larger area of the leg remains numb after the operation as a result of the internal saphenous nerve being stretched. Feeling is usually recovered within 6 months. More rarely, the loss of feeling persists but is not bothersome.
If you have any concerns about the operation, do not hesitate to talk to your surgeon or the anaesthetist and they will answer any questions you may have.